No matter where and when you got your sex education, you likely heard some incorrect information, whether it be from friends, parents, pop culture, the media, or formal education. If you learned false information about sex, we are here to help.
Generalizations are often made leaving some to feel confused or harmed by the information given to them. Today on the Embrace Sexual Wellness blog, we will be debunking some of the myths you may have learned about sex.
Myth #1: Orgasm is the be-all-and-end-all of sex
Having an orgasm can be a wonderful sensation, but it does not have to be the goal of all sexual interactions. Sex is so much more than the moment of orgasm. It is about pleasure and connection with your partner(s). Consider this, what would it be like if you thought about sexual pleasure as a journey and not a destination?
Thinking about orgasm as the goal of sex can also lead to increased stress, not pleasure. According to a study published in Hippokratia, when one feels pressure to perform sexually, their body activates its sympathetic nervous system, which results in the increased production of stress hormones, such as epinephrine, norepinephrine and cortisol. These hormones increase blood pressure levels and reduce blood flow to the genitals, which can lead to sexual functioning problems (e.g., decreased sensation in the vulva, erectile dysfunction, inhibited arousal), as well as a more stressful sexual dynamic between partners.
Orgasms are not a given in all sexual interactions and this pressure to perform can lead to added stress. A 2020 study in Current Sexual Health Reports notes that the orgasm gap still exists. The orgasm gap is the phenomenon that in heterosexual relationships, male partners orgasm at higher rates than their female counterparts. Furthermore, the experience of orgasm can be limiting. A theory in an article published in Current Sexual Health Reports states that those with penises are more likely to reach orgasm since they are taught from a young age that it is okay to explore their bodies more than those with vulvas. Additionally, the research suggests that the cultural prioritization of penile-vaginal intercourse over more clitorally focused sexual activities is linked to the orgasm gap.
Furthermore, an article in Healthline emphasizes the importance of pleasure during sex aside from an orgasm. The article also notes that when focusing on achieving orgasm alone, safety, well-being, respect, and connection are neglected.
TLDR: Orgasms are wonderful, but they are not the be-all-and-end-all.
Myth #2: Sex = vaginal penetration
The heteronormative idea that sex is simply vaginal penetration is incorrect. According to Teen Health Source, a Planned Parenthood Canadian-run sexual health information service for teens, the definition of sex is flexible. Being sexual means different things to different people, and only you get to decide how you define being sexual. Sex can include a range of activities that feel sexual and pleasurable to you.
Research inspired by Alfred Kinsey that was published in PLOS ONE, indicates that there are many common sexual behaviors including but not limited to vaginal sex, oral sex, anal sex, sending and receiving nude images, and masturbation. Assuming that sex is only vaginal penetration is exclusionary to those who do not have vaginal sex, or cannot for health reasons. By expanding our definitions of sex, we can make sex more inclusive to people across all identities.
Myth #3: A person with a vulva pops their cherry when they have sex for the first time
Did you ever hear the phrase “popping one’s cherry”? The phrase popping your cherry tends to apply to the belief that an intact hymen is an indicator if someone with a vulva has engaged in vaginal intercourse. According to an article in Women’s Health Magazine, many still believe that an intact hymen is a sign of purity. Well, guess what? Popping one’s cherry is not an accurate phrase in determining if someone has engaged in vaginal intercourse or is “pure”.
The hymen is a membrane that lines the opening of the vagina and varies in its size and shape. According to Medical News Today, many people with vulvas do not experience tearing of the hymen during sexual intercourse and sometimes hymens are torn during other non-sexual physical activities, such as horseback riding, riding bicycles, gymnastics, and inserting tampons. In fact, according to a study published in the North American Society for Pediatric and Adolescent Gynecology, some people with vaginas do not have hymen to begin with which means that they never will “pop their cherry”.
A person does not “pop their cherry” and a “popped cherry” does not mean a person is no longer pure. There has never been validity to these messages.
Myth #4: Virginity is an accurate concept (CW: Sexual Violence and Racism)
In her book Virgin: The Untouched History, Hanne Blank, shares that humans have constructed the idea of virginity. This concept, that almost always focuses on females in heterosexual sexual encounters, has been used as an exploitative force for political and cultural forces. In fact, in the Renaissance and Medieval periods, western virginity was symbolized by whiteness and nonwhite people were viewed as sexually immoral. European colonizers also used the concept of virginity to sexually abuse Black women. A 2016 article published in Black & Gold, discusses how Black women were hyper sexualized by white men in order to justify raping and dehumanizing them. The idea of virginity was critical in this historical narrative to justify that white women were pure while Black women were viewed as impure.
The concept of virginity is problematic because it teaches women that their virginity (a.k.a. their sexual behavior) is a commodity for men. Women are often shamed for being sexual, a.k.a. “losing their virginity”, while men are praised for doing so. This sexist ideology that it is okay for men to have sex, but not for women can lead to slut-shaming.
Virginity is important to some people who choose to engage in abstinence (often defined as waiting to have sex until marriage) or secondary abstinence (waiting to have sex until marriage after having sex prior). According to a study published in Sexuality & Culture, secondary virginity is based on the social construction of gendered sexuality and heterosexuality. This idea of secondary virginity is often infused with conservative Christian ideology, but for some, it is simply a method to protect against pregnancy and STIs. For others, it is a commitment to wait until they are emotionally connected to someone, in some cases waiting to have sex until marriage.
The term ‘virgin’ is typically used to describe a person who has never had sex, but this is also challenging since the definition of sex is ambiguous. According to Planned Parenthood, the concept of virginity is inaccurate because everyone defines sex differently and the term is not helpful in determining if someone was sexually active or not. Only you can decide if you are a virgin, but it doesn’t need to matter or hold value unless you want it to. Sexuality professionals recommend using less loaded terms such as ‘sexual debut’ or ‘first sexual encounter’. According to Healthline, this myth of virginity can impact the way we think about sex and our expectations for sex in the first place. The concept of virginity as we know it assumes that one is losing something when they have sex for the first time, putting a negative connotation on sex.
Myth #5: The words vulva and vagina are interchangeable
This is something a lot of people misunderstand, including people with vulvas. Planned Parenthood defines the vulva as the part of the genitals on the outside of the body of those who were assigned female at birth. The vagina, however, is a canal that connects one’s vulva with their cervix and uterus. It’s the portal to which babies and menstrual blood leave the body. Vaginas are one part of the vulva, which is the larger structure.
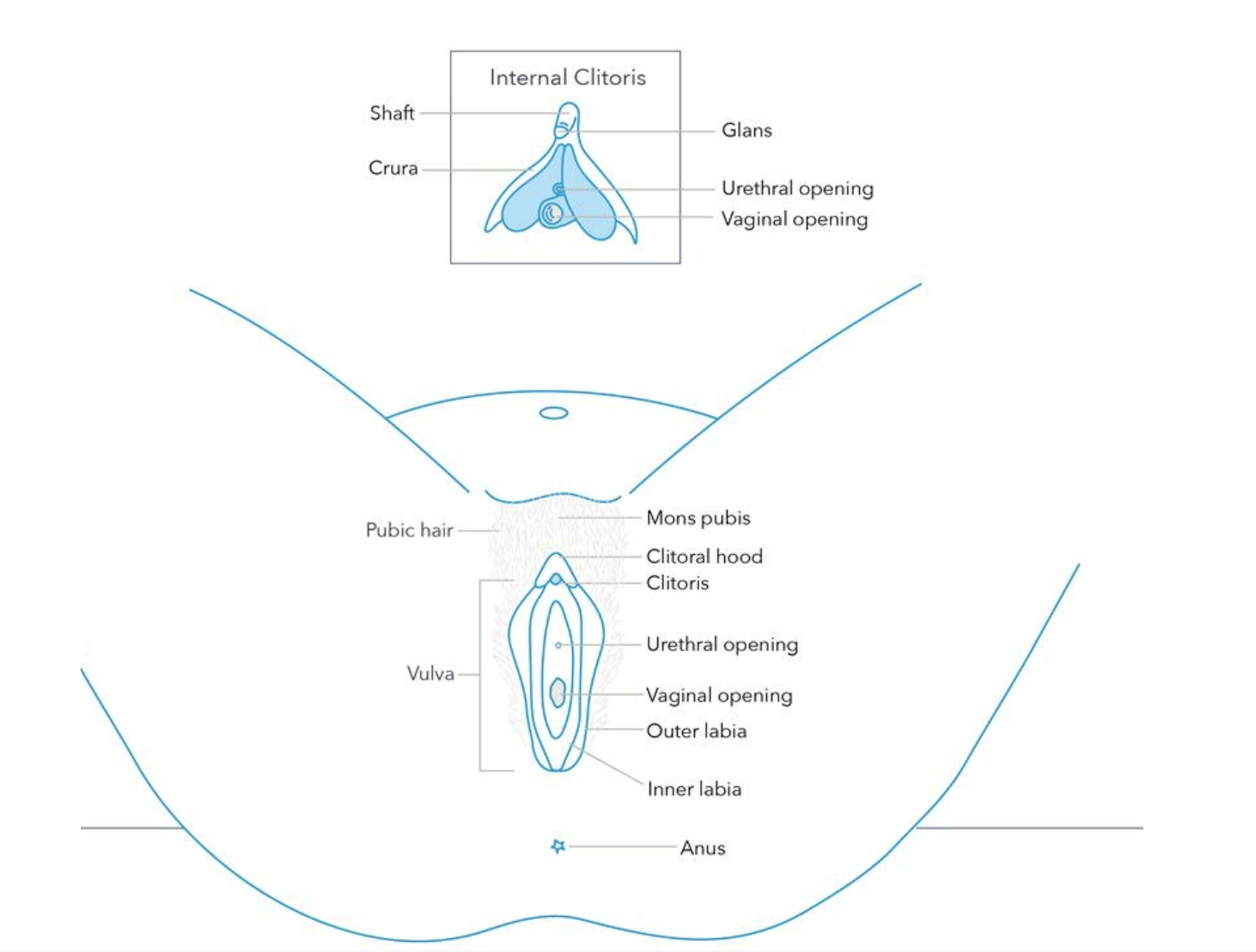
Source: Planned Parenthood
Myth #6: People with disabilities and chronic illnesses cannot have sex
People with disabilities and chronic illnesses are sexual beings. The myth that they cannot have sex or are not sexual largely stems from ableism. Our Bodies, Ourselves, an organization that empowers women with information about health, sexuality and reproduction, debunks this myth that those with chronic illness and disabilities are uninterested in sex, unable to have sex, or are undesirable. In fact, they indicate that some women with chronic illness, such as fibromyalgia, find that direct genital stimulation can help block the pain that they are feeling. They also note that medical establishments need to recognize that people with chronic illness and disabilities want to be seen as sexual beings. A study published in American Family Physician specifies that this assumption can be harmful to those with disabilities and chronic illnesses, as it can cause them to become uninterested in sex because of misconceptions about their ability to have sex, as well as other factors, such as depression, fatigue, pain and stress.
Myth #7: Sex ends with ejaculation
Absolutely not! Sexual interactions are about the pleasure of all parties involved. It is important to communicate with your partner(s) about when you are ready for sex to be over. Partnered sex is about communal pleasure. Unless you are engaging in a specific BDSM scene where one person’s pleasure is prioritized over another, such as in a M/S dynamic, and it has been decided beforehand, everyone’s pleasure should be prioritized.
Pleasure is the cornerstone of sexual wellbeing. Ejaculation is not. All bodies are different and not all bodies will always ejaculate during sex. Everyone’s pleasure is important!
Myth #8: The pullout method is an effective way to prevent pregnancy
This myth is one that affects people who are engaging in penile-vaginal intercourse, which is not reflective of all sexual interactions. The pullout method is a method of birth control where the partner with a penis removes their penis from the vagina before ejaculation occurs. Some may believe that the pullout method is a reliable and effective method of birth control, when in fact it is not. According to Planned Parenthood, the pullout method, also known as withdrawal, is only 78% effective when used alone. Furthermore, the pullout method does not work to protect against STIs. Barrier methods such as internal and external condoms and dental dams are safer methods that can effectively prevent pregnancy and the transmission of STIs and HIV.
Myth #9: Kink is shameful
Kink is not shameful. It is actually extremely common. An article published in Haworth Press reveals that up to 14% of American men and 11% of American women report having engaged in some form of BDSM. The Kink Clinical Practice Guidelines also state that approximately 45-60% of the population experience fantasies related to dominance and/or submission. By understanding how common kink is, we can begin to break down the stigma surrounding kink and those that practice it.
Kink is also not a monolith. When shaming the world of kink, many are shaming a concept, rather than an act. There are multiple ways to engage in kink, such as bondage, dominance, masochism, submission, and role play, and none of them are shameful. Give this Glamour article a read to learn more about kinks and fetishes in A to Z format.
Research published in the Journal of Sex Medicine suggests that people who practice kink have a desire to engage in discussions with their health care providers about their health without fear of being judged for their sexual desires. The more that kink is societally stigmatized, the more harmful it can be to those engaging in kink.
TLDR: Kink is not shameful and Kinksters should not be stigmatized. A kink is simply a form of sexual desire or behavior.
Takeaway
While these are not the only myths and misconceptions about sex, these are some of the common ones we have heard frequently. It is always good to do your research before believing something new about sex, or anything for that matter. There is so much false information, and we are here to help. Some things you can do when encountering new information about sex include: consider the source of the information, research the information yourself and look for empirical evidence that supports or disproves it, and talk with professionals about why said information is fact versus opinion.
Remember, sexuality education is a lifelong journey. Looking for more resources to continue learning? Visit our resources page here to learn more.